By continuing to use our site, you consent to the processing of cookies, user data (location information, type and version of the OS, the type and version of the browser, the type of device and the resolution of its screen, the source of where the user came from, from which site or for what advertisement, language OS and Browser, which pages are opened and to which buttons the user presses, ip-address) for the purpose of site functioning, retargeting and statistical surveys and reviews. If you do not want your data to be processed, please leave the site.
The Voice of People With Breast Cancer
Information
Treatments & Side Effects
Surgery
Breast cancer surgery is a key part of treatment and also provides valuable information about tumour grade and stage. This helps guide further treatments, such as chemotherapy, hormone therapy, or radiation therapy. Surgery may be performed to:
- Remove the cancer entirely
- Treat a cancer that has come back in the same area (known as local recurrence)
- Check and remove lymph nodes
- Help with breast reconstruction
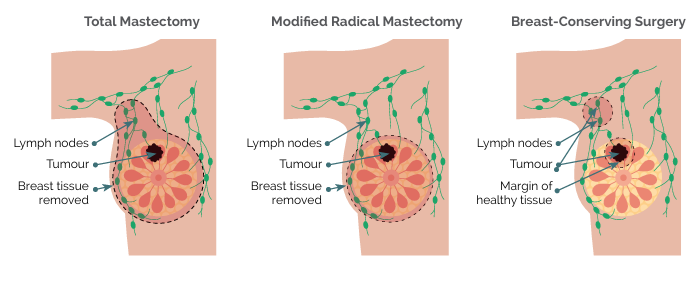
The two main types of breast cancer surgery are lumpectomy (breast-conserving surgery) and mastectomy.
Lumpectomy (breast-conserving surgery)
A lumpectomy removes the tumour along with a margin of surrounding healthy tissue, allowing the breast to be preserved. Studies show that for early-stage breast cancer (tumours 4 cm or smaller), lumpectomy followed by radiation therapy is as effective as mastectomy in preventing recurrence.
This surgery is typically recommended for:
- Early-stage breast cancer, when the tumour is small and confined to the breast
- Tumours that can be removed without significantly changing the shape or appearance of the breast
- Small or limited ductal carcinoma in situ (DCIS), which is a non-invasive form of breast cancer
- People who want to keep their breast and are able to have radiation therapy after surgery
- Tumours located in one part (quadrant) of the breast, rather than in multiple separate parts of areas
After most breast-conserving surgeries, radiation therapy is recommended to reduce risk of recurrence.
Mastectomy
A mastectomy involves the surgical removal of the entire breast and may be recommended for:
- People with larger or multiple tumours
- Those who cannot have radiation therapy
- Individuals at high risk who opt for complete breast removal
- People with inflammatory breast cancer
- People who are at high genetic risk and who have breast cancer
Types of mastectomies:
- Total (simple) mastectomy: Removes the entire breast, including the nipple and areola, but does not remove lymph nodes. Used for DCIS and preventive mastectomy.
- Modified radical mastectomy: Removes the entire breast and some or all of the axillary (underarm) lymph nodes. Used for inflammatory breast cancer.
- Skin-sparing mastectomy: Preserves most of the breast skin for easier reconstruction. Recommended for early-stage cancers.
- Nipple-sparing mastectomy: Removes breast tissue but leaves the nipple and areola intact. Suitable for selected patients.
- Double (bilateral) mastectomy: Removes both breasts, often for those with high genetic risk (e.g., BRCA1/BRCA2 mutation carriers).
Mastectomy recovery takes longer than a lumpectomy, with a higher risk of complications. Some people choose a mastectomy for peace of mind, even when a lumpectomy would be just as safe and effective in treating their cancer. It is important to note that choosing mastectomy over a lumpectomy for early breast cancer does not improve survival, meaning it does not decrease the chance of dying of breast cancer.
Post-mastectomy options
After a mastectomy, people may choose from the following options:
- Breast implants: filled with saline or silicone to recreate the shape of the breast
- Autologous reconstruction: uses tissue from another part of the body
- Aesthetic flat closure: a surgical closure that creates a smooth, flat chest instead of rebuilding the breast
- External breast prosthesis: a removable breast form worn inside a bra
Factors influencing surgical decisions
Choosing between breast-conserving surgery and mastectomy depends on several factors:
- Personal choice: Some opt for mastectomy for peace of mind, while others prefer to keep as much of their breast as possible.
- Tumour size and location: Larger tumours or multiple tumour sites may require mastectomy.
- Breast size: If the tumour is large compared to the size of the breast, a mastectomy may be needed.
- Genetic risk factors: People with BRCA1/BRCA2 mutations may consider a preventative (known as prophylactic) mastectomy to lower their risk of developing another breast cancer in the future.
- Radiation therapy suitability: Lumpectomy is typically followed by radiation. If radiation is not an option, mastectomy may be recommended.
Prophylactic mastectomy
A prophylactic (preventive) mastectomy is performed to reduce the risk of developing breast cancer in people with a high genetic or familial risk. It is considered for:
- People with BRCA1, BRCA2, or other genetic mutations
- A strong family history of breast cancer in selected cases
Lymph node surgery
Lymph nodes play a key role in filtering cancer cells that may have spread beyond the breast. Surgeons often remove lymph nodes from the armpit to check for cancer presence.
Types of lymph node surgery include:
- Sentinel lymph node biopsy (SLNB): Removes a few key lymph nodes closest to the breast, the most likely to have cancer cells if they have spread.
- Axillary lymph node dissection (ALND): A more extensive procedure that removes multiple lymph nodes, typically performed when there are cancer cells in the nodes and can be felt during a clinical examination.
- Targeted axillary dissection (TAD): Removes 1 or 2 lymph nodes that have been biopsied before surgery and contain a metallic clip to identify them.
Lymph node surgery is often done at the same time as a mastectomy or a lumpectomy. The results help determine further treatment options.
Surgery in men with breast bancer
Men with breast cancer typically have a mastectomy, as they have less breast tissue. Lymph node removal may also be performed. Lumpectomy and breast reconstruction is less common but available for those who desire it.
If you are deciding what type of surgery and reconstruction options to pursue, visit our SurgeryGuide decision aid to help you make a choice you can feel confident about.
Medical Review by Mark Basik, MD, FRCSC, December 2025
- References
-
American Cancer Society. (2023). Surgery for breast cancer. Cancer.org. https://www.cancer.org/cancer/types/breast-cancer/treatment/surgery-for-breast-cancer.html
Canadian Breast Cancer Network. (2022). Breast cancer and you: A guide for people living with breast cancer [PDF]. https://cbcn.ca/web/default/files/public/Reports/Breast%20Cancer%20and%20You_ENG_edit_web.pdf
Canadian Breast Cancer Network. (2025). Surgery guide. https://www.cbcn.ca/en/surgeryguide
Canadian Cancer Society. (2024). Choosing the breast surgery that is right for you. https://cancer.ca/en/cancer-information/cancer-types/breast/treatment/surgery/choosing-the-breast-surgery-that-is-right-for-you
Canadian Cancer Society. (2024). Surgery for breast cancer. https://cancer.ca/en/cancer-information/cancer-types/breast/treatment/surgery
Czajka, M. L., & Pfeifer, C. (2023). Breast cancer surgery. In StatPearls. StatPearls Publishing.
Hofvind, S., Holen, Å., Aas, T., Roman, M., Sebuødegård, S., & Akslen, L. A. (2015). Women treated with breast conserving surgery do better than those with mastectomy independent of detection mode, prognostic and predictive tumor characteristics. European Journal of Surgical Oncology: The Journal of the European Society of Surgical Oncology and the British Association of Surgical Oncology, 41(10), 1417–1422. https://doi.org/10.1016/j.ejso.2015.07.002
SHARE
Our Stories

Events
 Receive updates by email Subscribe Now
Receive updates by email Subscribe Now
About CBCN
CBCN strives to voice the views and concerns of breast cancer patients through education, advocacy activities, and the promotion of information sharing.
Canadian Breast Cancer Network
185 Somerset St. West Suite 318, Ottawa, ON Canada K2P 0J2
Tel: 613-230-3044
Toll-free: 1-800-685-8820
Email Us


